- Search Engine
- Online Advertisement
- Referral
- TikTok
- Artas
- Newsday
- Other
- No elements found. Consider changing the search query.
- List is empty.
- Right Away
- 1-3 Months
- 3-6 Months
- 6-12 Months
- 12 +
- I'm not sure, I know I need something
- No elements found. Consider changing the search query.
- List is empty.
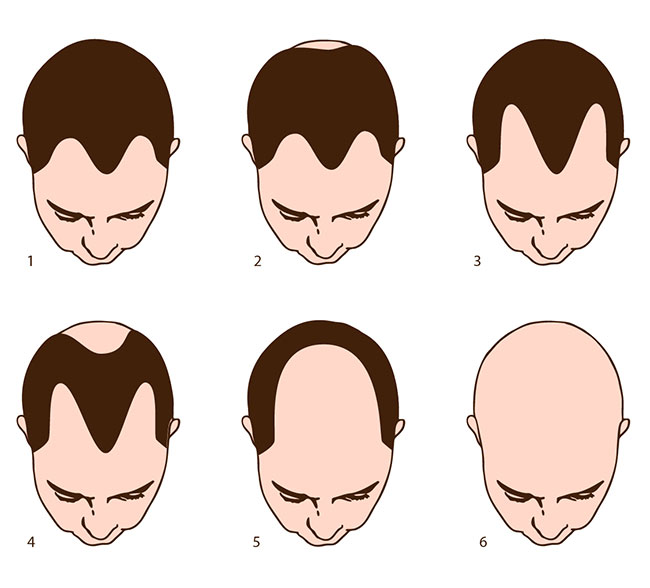
Using the image below for reference, please select which hairline most resembles yours
Select one
- 1
- 2
- 3
- 4
- 5
- 6
- No elements found. Consider changing the search query.
- List is empty.