
Dental Record Chart
Note: If you don't follow instructions (e.g. incomplete full name), it will be not entertained or automatically refuse to consultation
We’ll send your dental certificate and prescription to this email address — make sure it’s correct!
Medical History
if nt applicable please put N/A
if nt applicable please put N/A
Dental History
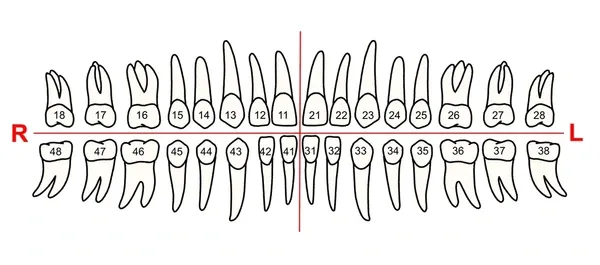
Please use the Image below as your reference (e.g. i have tooth ache and cavity on tooth #12); Please be specific on what tooth you concern.
If not applicable, please input the date today
Put N/A if not applicable
N/A if not applicable
Note: reason must be valid or true or else, it will be subjected to rejection of your dental certificate.
e.g, From Jan 1 to 2
Optional
Leave it if you don't have
Picture of your mouth/teeth invloved/proof of your main concern if you have