
ACH AUTHORIZATION FORM
Carrier & Policy Information
Bank Account Holder
Please complete this form to authorize Peak Insurance to make a payment using your Bank Account (ACH Payment) directly to the Insurance Carrier.
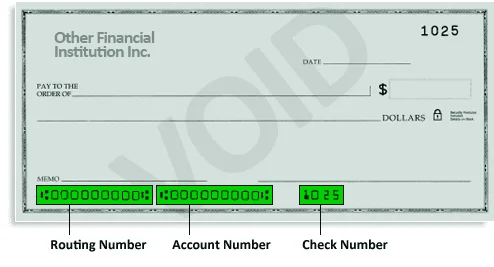
must be 9 numbers - no spaces
must be 9-12 numbers - no spaces
City, State
Example: Personal Checking, Business Checking
Authorization To Withdraw Payment
I authorize Peak Insurance to initiate an ACH payment from my bank account as specified above, on my behalf, to the designated insurance carrier for the purpose of paying my insurance premium.
I understand this authorization is valid for one-time use only. I acknowledge that I am responsible for ensuring sufficient funds are available in my account for this transaction.
Authorization
$
