
New Patient Health History Intake Form
Patient Information
- Single
- Married
- Divorced
- Widower/Widowed
- In a domestic partnership
- No elements found. Consider changing the search query.
- List is empty.
Motor Vehicle Accident Details
- Yes
- No
- No elements found. Consider changing the search query.
- List is empty.
- Driver
- Front Passenger
- Rear Driver Passenger
- Rear Passenger
- No elements found. Consider changing the search query.
- List is empty.
- Front
- Rear
- Left Side
- Right Side
- Left Front Quarter Panel
- Right Front Quarter Panel
- Left Rear Quarter Panel
- Right Rear Quarter Panel
- No elements found. Consider changing the search query.
- List is empty.
- Street
- Parking Lot
- Stop Sign
- Intersection
- Highway
- No elements found. Consider changing the search query.
- List is empty.
- Forward
- Left
- Right
- Left (in reverse)
- Right (in reverse)
- No elements found. Consider changing the search query.
- List is empty.
- Yes
- No
- No elements found. Consider changing the search query.
- List is empty.
- Yes
- No
- No elements found. Consider changing the search query.
- List is empty.
- Yes
- No
- No elements found. Consider changing the search query.
- List is empty.
- Yes
- No
- No elements found. Consider changing the search query.
- List is empty.
Auto Insurance Information
Chief Complaints
Primary Complaint
- 0 - None
- 1 - Mild
- 2 - Mild
- 3 - Mild
- 4 - Moderate
- 5 - Moderate
- 6 - Moderate
- 7 - Severe
- 8 - Severe
- 9 - Severe
- 10 - Severe
- No elements found. Consider changing the search query.
- List is empty.
- Occasionally (0%-25% of the time)
- Intermittently (25%-50% of the time)
- Frequently (50%-75% of the time)
- Constantly (75%-100% of the time)
- No elements found. Consider changing the search query.
- List is empty.
- AM
- PM
- Mid-Day
- Afternoon
- Late PM
- No elements found. Consider changing the search query.
- List is empty.
- Yes
- No
- Unknown
- No elements found. Consider changing the search query.
- List is empty.
- Yes
- No
- No elements found. Consider changing the search query.
- List is empty.
- Work
- Home
- Relationships
- Daily Routine
- Sleep
- Recreation
- No elements found. Consider changing the search query.
- List is empty.
- Sitting
- Standling
- Walking
- Bending
- Lifting
- Laying Down
- Reaching
- No elements found. Consider changing the search query.
- List is empty.
Secondary Complaint
- Occasionally (0-25% of the time)
- Intermittently (25%-50% of the time)
- Frequently (50%-75% of the time)
- Constant (75%-100% of the time)
- No elements found. Consider changing the search query.
- List is empty.
- AM
- PM
- Mid-Day
- Afternoon
- Late PM
- No elements found. Consider changing the search query.
- List is empty.
- Yes
- No
- Unknown
- No elements found. Consider changing the search query.
- List is empty.
- Work
- Sleep
- Recreation
- Daily Routine
- No elements found. Consider changing the search query.
- List is empty.
- Sitting
- Standing
- Walking
- Bending
- Lifting
- Laying Down
- Reaching
- No elements found. Consider changing the search query.
- List is empty.
Third Complaint
- 0
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- No elements found. Consider changing the search query.
- List is empty.
- Occasionally (0-25% of the time)
- Intermittently (25%-50% of the time)
- Frequently (50%-75% of the time)
- Constant (75%-100% of the time)
- No elements found. Consider changing the search query.
- List is empty.
- AM
- PM
- Mid-Day
- Afternoon
- Late PM
- No elements found. Consider changing the search query.
- List is empty.
- Yes
- No
- Unknown
- No elements found. Consider changing the search query.
- List is empty.
- Work
- Sleep
- Recreation
- Daily Routine
- No elements found. Consider changing the search query.
- List is empty.
- Sitting
- Standing
- Walking
- Bending
- Lifting
- Laying Down
- Reaching
- No elements found. Consider changing the search query.
- List is empty.
_________________________________________________________________________________________________________
Have you ever been diagnosed or told you had any of the following?
Review of Systems
Please select the appropriate box for any of the following symptoms you HAVE or previously HAD.
GENERAL
MUSCLE & JOINT
GASTRO-INTESTINAL
EYES, EARS, NOSE & THROAT
CARDIOVASCULAR
RESPIRATORY
SKIN
GENITOURINARY
* WOMEN ONLY *
- Yes
- No
- N/A
- No elements found. Consider changing the search query.
- List is empty.
__________________________________________________________________________________________________________
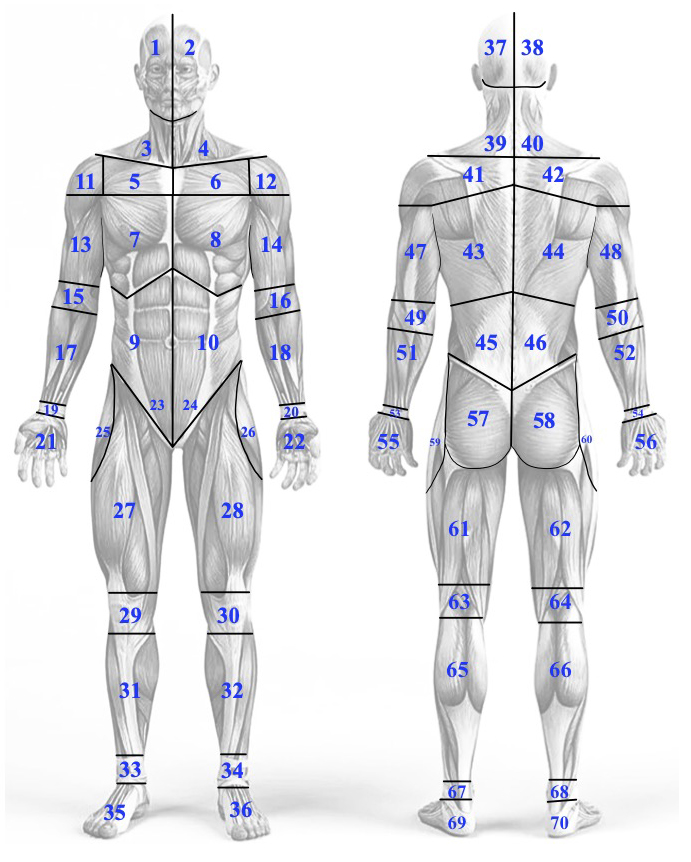
Select the number(s) below that correspond to the complaint area(s) shown in the graphic above.
FRONT of the Body:
BACK of the Body:
_________________________________________________________________________________________________________
Assignment of Benefits, Letter of protection, & Lien
I, the undersigned (hereinafter referred to as "Patient"), and Chiropractic Solutions of Georgia, LLC, doing business as Douglas Family Chiropractic, enter into this AGREEMENT on the date below. This agreement includes a Letter of Protection, Lien, and Assignment of Benefits.
WHEREAS Patient desires to receive medical/rehabilitative services from Chiropractic Solutions of Georgia, LLC., and in consideration for awaiting payment for such services, desires to assign certain rights and benefits to Chiropractic Solutions of Georgia, LLC.
ACCORDINGLY, it is hereby agreed:
Patient assigns to Chiropractic Solutions of Georgia, LLC., any and all benefits payable by Patient’s insurance or health care plans as a result of charges incurred by Patient for services rendered by Chiropractic Solutions of Georgia, LLC. Patient also assigns to Chiropractic Solutions of Georgia, LLC., any and all contractual rights Patient has against any insurance company, health care benefit plan or other party liable to Patient for payment of health care costs incurred as a result of services rendered by Chiropractic Solutions of Georgia, LLC.
Patient understands that he/she is fully and ultimately responsible to Chiropractic Solutions of Georgia, LLC., for payment of all services rendered, and that this agreement is made solely for additional protection and consideration for awaiting payment. Patient understands that responsibility for such payment is not contingent on any settlement, claim, judgment or verdict which Patient and /or his/her attorney may recover.
Patient understands that this assignment and letter of protection grants a lien to Chiropractic Solutions of Georgia, LLC., and is irrevocable.
Patient directs all insurers and other persons responsible for Patient’s health care costs to make payment for services rendered directly to:
Chiropractic Solutions of Georgia, LLC. dba Douglas Family Chiropractic
610 Shorter Ave. NW, Suite 9
Rome, GA 30165
Patient authorizes Chiropractic Solutions of Georgia, LLC., to submit a copy of this agreement as notice of its lien to any insurance company, health care benefit plan, attorney or other party liable to Patient for payment of health care costs incurred as a result of this accident, for services rendered by Chiropractic Solutions of Georgia, LLC.
Patient authorizes Chiropractic Solutions of Georgia, LLC., to provide his/her attorney a copy of this document as notice of Chiropractic Solutions of Georgia, LLC’s lien for services rendered in the event of a recovery related to the services. Patient further understands that his/her attorney will be bound by this lien and treat it as an assignment of benefits and letter of protection for monies due to Chiropractic Solutions of Georgia, LLC., for services rendered as a result of below accident.
Patient agrees to promptly notify Chiropractic Solutions of Georgia, LLC., of any change or addition of attorney(s), if any, used in connection with this incident.
A copy of this document shall be binding as the document bearing the original signatures.
__________________________________________________________________________________________________________
Terms of Consent & Acceptance
You are the decision maker for your health care. Part of our role is to provide you with information to empower you to make informed choices. The process is often referred to as "informed consent". It involves your understanding and agreement regarding the care we recommend, the benefits and risks associated with the care, alternatives, and the potential effect on your health if you choose not to receive the care.
We may conduct some diagnostic or examination procedures if indicated. Any examinations or tests conducted will be carefully performed but may be uncomfortable.
Chiropractic care centrally involves what is known as a chiropractic adjustment. There may be additional supportive procedures or recommendations as well. When providing an adjustment, we use our hands or an instrument to reposition anatomical structures, such as vertebrae. Potential benefits of an adjustment include restoring normal joint motion, reducing swelling and inflammation in a joint, reducing pain in the joint, and improving neurological functioning and overall well-being.
It is important that you understand, as with all healthcare approaches, that results are not guaranteed, and there is no promise to cure. As with all types of health care interventions, there are some risks to care, including, but not limited to, muscle spasms, aggravating and/or temporary increase in symptoms, lack of improvement of symptoms, burns and/or scarring from electrical stimulation and from hot or cold therapies, including but not limited to hot packs, and ice, fractures (broken bones), disc injuries, strokes, dislocations, strains, and sprains. With respect to strokes, there is a rare but serious condition known as an "arterial dissection" that typically is caused by a tear in the inner layer of the artery that may cause the development of a thrombus (clot with the potential to lead to a stroke). The best available scientific evidence supports the understanding that chiropractic adjustment does not cause a dissection in a normal, healthy artery. Disease processes, genetic disorders, medications, and vessel abnormalities may cause an artery to be more susceptible to dissection. Strokes caused by arterial dissections have been associated with over 72 everyday activities, such as sneezing, driving, and playing tennis.
Arterial dissections occur in 3-4 of every 100,000 people, whether they are receiving health care or not. Patients who experience this condition often, but not always, present to their medical doctor or chiropractor with neck pain and headache. Unfortunately, a percentage of these patients will experience a stroke.
The reported association between chiropractic visits and stroke is exceedingly rare and is estimated to be related to one in one million to one in two million cervical adjustments. For comparison, the incidence of hospital admission attributed to aspirin use from major GI events of the entire (upper and lower) GI tract was 1219 events/ per one million persons/year, and the risk of death has been estimated as 104 per one million users.
It is also important that you understand there are treatment options available for your condition other than chiropractic procedures. You have likely tried many of these approaches already. These options may include, but are not limited to: self-administered care, over-the-counter pain relievers, physical measures and rest, medical care with prescription drugs, physical therapy, bracing, injections, and surgery. Lastly, you have the right to a second opinion and to secure other opinions about your circumstances and health care as you see fit.
I have read, or have had it read to me, the above consent. I appreciate that it is not possible to consider every possible complication in care. I have also had an opportunity to ask questions about its content, and by signing below, I agree with the current or future recommendations to receive chiropractic care as is deemed appropriate for my circumstance. I intend this consent to cover the entire course of care from all providers in this office for my present condition and for any future condition(s) for which I seek chiropractic care from this office.
No-Show/Cancellation Policy
Our mission is to provide high-quality, practice-member-centered care that addresses root causes and allows practice members to thrive. Due to our high volume of practice members and the desire to accommodate both our members and providers, we ask that you give the office 24 business hours' notice before canceling or rescheduling your appointments.
A No-Show or cancellation with less than 24 hours notice significantly limits our ability to make the appointment available for another patient in need.
To remain consistent with our mission, we have instituted the following policy:
Please give our office 24 hours notice if you need to reschedule your appointment. This will allow us to provide care to another Practice Member.
A "No-Show," "No-Call," or missed appointment without proper 24-hour notification will be assessed a $175 fee.
This fee is not billable to your insurance.
If you are 15 or more minutes late for your appointment, the appointment may be canceled and rescheduled.
As a courtesy, we send reminder texts for appointments in advance. Please note that the cancellation policy remains in effect if a reminder call or message is not received.
More than three missed appointments may result in termination of care.
If you have any questions regarding this policy, please let our staff know; we will gladly clarify them.
_________________________________________________________________________________________________________
HIPAA Notice
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
WHO IS COVERED BY THIS NOTICE
This notice describes the privacy practices of the affiliated physician practice plans of Chiropractic Solutions of Georgia, LLC., dba Douglas Family Chiropractic including:
Any health care professional authorized to enter information into your medical record.
All employees and staff at Chiropractic Solutions of Georgia, LLC. dba Douglas Family Chiropractic
OUR PLEDGE REGARDING MEDICAL INFORMATION
We are required by law to:
make sure that your health information is kept private;
give you this notice of our legal duties and privacy practices; and
follow the terms of the notice that is currently in effect.
We understand that your health information is personal. We create a record of the care and services you receive. We need this record to provide you with quality care and to comply with certain legal requirements. We are committed to protecting this information.
This notice will tell you about:
the ways in which we may use and disclose your health information
your rights; and
our obligations regarding the use and disclosure of health information
HOW WE MAY USE AND DISCLOSE YOUR HEALTH INFORMATION
We may use or share your health information in certain ways. We will explain how and when we may use or share your health information. We are not able to list each specific way we may use or share your health information, but each situation will fall into one of the basic types of situations below:
For Treatment. It is important that we be able to use or share your information to treat you. We may share your information with doctors, nurses, technicians, medical students, or other personnel who are involved in taking care of you. We may share your information with healthcare providers for your treatment.
For example, a doctor treating you for a broken leg may need to know if you have diabetes because diabetes may slow the healing process. We may need to share your information in order to schedule you for surgery or a procedure. A healthcare provider may need to know about any drug allergies that you have in order to provide you with appropriate medication.
For Payment We may use or share your health information so that we are paid for the cost of your care. We may share your information with another provider so that they may be paid for services as well. We may bill, and share information with other providers, an insurance company, you, or a third party.
For example, we may need to give your health plan information about your diagnosis and treatment so your health plan will pay us or reimburse you for the care we provide. We may also tell your health plan about a treatment you are going to receive to obtain prior approval or to determine whether your plan will cover the treatment. We may also share your health information in order to facilitate payment to another provider who has participated in your care.
Health-Related Benefits and Services We may use and disclose medical information to tell you about treatment options, health-related benefits, or services that may be of interest to you.
Individuals Involved in Your Care or Payment for Your Care We may release medical information about you to a family member or other designated person who is involved in your medical care. We may also give information to someone who helps pay for your care.
For example: We may need to tell the person who comes to pick you up after the appointment what he or she may need to do to help you once you get home.
In the event of an emergency, we may need to use or share information about you in order to inform your family or persons responsible for your care where you are, and your condition. In addition, we may disclose medical information about you to an agency assisting in a disaster relief effort so that your family can be notified about your condition, status, and location.
SPECIAL SITUATIONS: Additional uses and disclosures for which authorization or opportunity to agree or object is not required by HIPAA.
Research It can help find cures for diseases and help you and many other people. Under certain circumstances, we may use and disclose medical information about you for research purposes. Often, you will need to give permission before we share your information with others for use in research. If your information is used, the researcher must keep your information safe and confidential.
As Required by Law We will disclose medical information about you when required to do so by federal, state, or local law.
To Avert a Serious Threat to Health or Safety We may use and disclose medical information about you when necessary to prevent a serious threat to your health and safety or the health and safety of the public or another person.
Workers' Compensation We may release medical information to Workers' Compensation, as required by workers’ compensation laws. This program provides benefits for work-related injuries or illnesses.
Public Health Risks As required by law, we may disclose your health information to public health authorities for purposes related to preventing or controlling disease, injury, or disability; reporting medical device safety issues and adverse events to the federal Food and Drug Administration’s MedWatch program; and reporting disease or infection exposure.
Victims of Abuse, Neglect, or Domestic Violence We may disclose certain health information to government agencies authorized by law to receive reports of abuse, neglect, or domestic violence if we believe that you have been a victim.
Health Oversight Activities We may disclose medical information to a health oversight agency for activities authorized by law. These oversight activities include, for example, audits, investigations, inspections, and licensure.
Judicial and Administrative Proceedings We may disclose your health information in the course of an administrative or judicial proceeding, such as in response to a court order
Law Enforcement We may release medical information to a law enforcement official if required or permitted by law.
Deceased Person Information We may release medical information to a coroner, medical examiner, or funeral director as necessary to carry out their duties.
Specialized Government Functions We may release medical information about you to authorized federal officials for national security and intelligence, military, or veterans’ activities required by law.
USES OF MEDICAL INFORMATION THAT REQUIRE AUTHORIZATION
In all other situations (situations that are not treatment, payment, health systems operations, or special situations, as we told you about above), we may only share information with your specific written authorization. You may revoke that authorization, in writing, at any time. If you revoke your permission, we will no longer use or disclose medical information about you for the reasons covered by your written authorization, except to the extent that we already have used or disclosed your information.
YOUR RIGHTS REGARDING MEDICAL INFORMATION ABOUT YOU
Although the physical form of your medical information or designated record set is our business record and is the property of the health system, the information contained in those records is your information, and you have certain rights regarding that information.
You have the following rights regarding medical information we maintain about you:
Right to Review and Copy You have the right to inspect and obtain a copy of medical information that may be used to make decisions about your care.
Usually, this information includes medical and billing records but does not include psychotherapy notes, information compiled for use in or created in anticipation of a civil, criminal, or administrative action or proceeding, or certain lab test results subject to the Clinical Laboratories Improvement Act of 1988. You must submit your request for your medical information in writing to the office manager of the office where you received your care. If you request a copy of the information, we may charge a fee for the costs of copying, mailing, or other supplies associated with your request.
Right to Appeal a Denial of Access to Medical Information You have the right to access your medical information. There are some limitations on that right. If for clear treatment reasons, your health provider has determined that access to your health information is likely to have an adverse effect on you, the health care provider shall provide the record to a practitioner designated by you to help you with your review of the information.
Your access is limited to your Designated Record Set. Your designated record set is the information we use to make decisions about your care. It does not include:
Information compiled for use in or created in anticipation of a civil, criminal, or administrative action or proceeding, or
Certain lab test results are subject to the Clinical Laboratories Improvement Act of 1988.
Other types of information that we did not use to make decisions about your health care.
Right to Amend If you feel that the medical information we have about you is incorrect or incomplete, you may ask us to amend the information. You have the right to request an amendment for as long as the information is maintained. We may deny your request if you ask us to amend information that:
is not part of the information which you would be permitted to inspect and copy; or
we believe is accurate and complete.
Submit your request to the office manager of the office where you received your care. Your request must be made in writing and include a reason that supports your request.
Right to an Accounting of Disclosures You have the right to request an accounting of disclosures. An accounting of disclosures is a listing of releases of your health information that we have made for the “Special Situations” listed in this Notice. We must document these disclosures and provide you with an accounting of them if we did not obtain your authorization before we released your information. You must submit your request in writing to the HIPAA Privacy Contact in the office where you were seen.
Your request must:
tell us the calendar dates you want to see. The time period cannot include more than six years of information, and cannot begin prior to April 14, 2003.
indicate in what form you want the list (paper copy or electronic).
Charges: There will be no charge for the first list you request within a 12-month period. We may charge you for the costs of providing any additional lists. We will notify you of the cost involved. You may choose to withdraw or modify your request at that time before any costs are incurred.
Right to Request Restrictions You have the right to request a restriction or limitation on the health information we use or disclose about you for treatment, payment, or health care operations. We are not required to agree to your request. If we do agree, we will comply with your request unless the information is needed to provide you with emergency treatment. You must make your request for any restrictions in writing to the office manager of the office where you received your care. In your request, you must tell us (1) what information you want to limit; (2) whether you want to limit our use, disclosure, or both; and (3) to whom you want the limits to apply (for example, disclosures to your spouse).
Right to Request Confidential Communications You have the right to request that we communicate with you about medical matters in a certain way or at a certain location. For example, you can ask that we only contact you at work or by mail. You must make your request for confidential communications in writing to the office manager where you received your care. We will not ask you why you are making this request. We will accommodate all reasonable requests. Your request must specify how or where you wish to be contacted. For example, if you wish to be contacted by telephone, be sure to provide an appropriate telephone number.
Right to a Paper Copy of This Notice You have the right to a paper copy of this notice. You may ask us to give you a copy of this notice at any time. Even if you have agreed to receive this notice electronically, you are still entitled to a paper copy of this notice. Contact a member of the office staff for a copy.
CHANGES TO THIS NOTICE We reserve the right to change this notice. We reserve the right to make the revised or changed notice effective for medical information we already have about you as well as any information we receive in the future. Current copies of this notice will be available at our office. The effective date of the notice is September 1, 2023.
COMPLAINTS If you believe your privacy rights have been violated, you may file a complaint with our health system by either contacting the Office Manager at the office where you received your care or with the U.S. Office of Civil Rights, Washington, DC. All complaints must be submitted in writing. You will not be penalized for filing a complaint.
HIPAA Acknowledgement
I give Chiropractic Solutions of Georgia, LLC. dba Douglas Family Chiropractic, permission to speak with the following people in regard to my care, appointments, insurance, billing, test results, claims etc. I acknowledge that the HIPAA policy is posted in the office and that I have read it. I understand that I can ask for a copy at any time.
_________________________________________________________________________________________________________
By signing below, I hereby authorize that all of the information stated about myself is truthful, and that I have read and agree to the above statements outlined in this form.