
Nutrition Questionnaire
Please read carefully and answer accurately. All fields marked with an * are required. Please put N/A if not applicable. Thank you!
Personal Details
Questions
GOALS
What is your 6 Week SMART Goal? (specific, measurable, achievable, relevant, and time-bound)
What is your lifetime goal?
Anything preventing from achieving those goals?
HEALTH HISTORY
Please provide a list of your past Injuries/surgeries/hospitalizations.
Any history with depression or anxiety?
Any other medical diagnosis?
Any other health concerns?
MEDICATIONS / SUPPLEMENTS
Do you have any active prescriptions? If yes, please list down the name and dose.
How frequent do you take your medication?
List any vitamins/supplements you take regularly.
GUT HEALTH
Please indicate the frequency of your bowel movements.
Please indicate the consistency of your bowel movements.
Any gut health concerns (GERD, IBS, etc)?
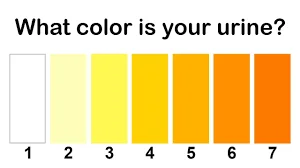
Select the number that corresponds to the color of your urine. (Please refer to the chart below)
SLEEP
How well do you sleep on a scale of 1-5? 5 being AWESOME.
How well do you fall asleep on a scale of 1-5? 5 being AWESOME.
How well do you stay asleep on a scale of 1-5? 5 being AWESOME.
Do you have a method for tracking sleep (Fitbit, Apple Watch, Oura Ring, etc)?
DIETARY RESTRICTIONS
Anything you can’t eat, won’t eat, don’t like, or are allergic to?
Habits/Behaviors
List down any habits/behaviors you don’t like & want to change?
Any habits/behaviors you wish you were doing but can’t seem to stick to?
What do you usually have for breakfast?
