Hair Implant Evaluation Form
Email (To match with your file)
*
Date of Birth - Hair Evaluation
Smoke nicotine or take controlled substances? Yes (list them) - Hair Implant Evaluation
What date have the procedure done? - Hair Implant Evaluation
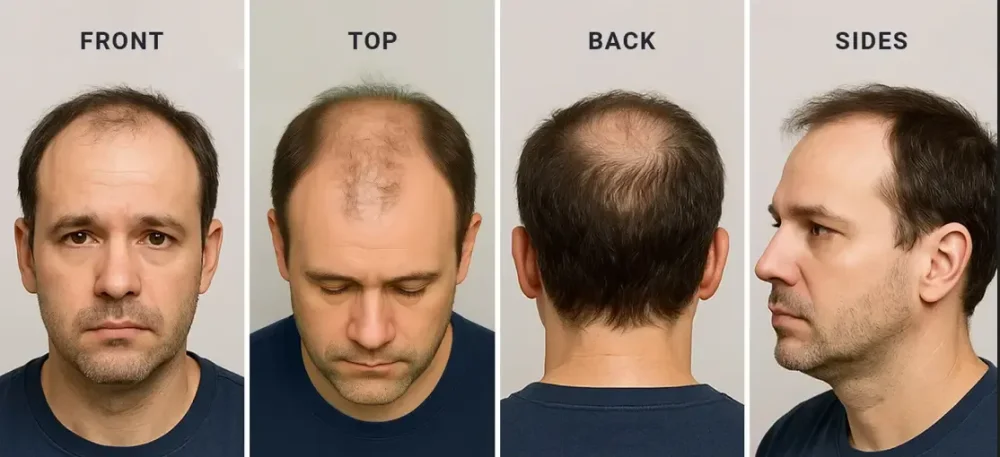
Top-down view - Hair Implant Evaluation
PNG, JPEG or JPG
Back of head - Hair Implant Evaluation
PNG, JPEG or JPG
Side profile - Hair Implant Evaluation
PNG, JPEG or JPG
Front view - Hair Implant Evaluation
PNG, JPEG or JPG
How long has the hair loss been progressing?
Hair loss worsening?
Yes
No
Areas to improve? (Check all)
Hairline
Crown
Temples
Top
Sides
Back
Overall density
Affected areas? (Check all)
Hairline
Crown
Temples
Top
Sides
Back
Goals? - Hair Implant Evaluation
Natural look
Maximum density
At what age did you first notice hair loss?
Medical conditions? Yes (list them) - Hair Implant Evaluation
Previous procedures? Yes (list them) - Hair Implant Evaluation
Drug allergies? Yes (list them) - Hair Implant Evaluation
Medications? Yes (list them) - Hair Implant Evaluation
Hospitalized in last 5 years? Yes (list them) - Hair Implant Evaluation
Fat burners/diet pills? Yes (list them) - Hair Implant Evaluation
Submit